Telehealth & Medicaid: A Fall 2021 Policy Webinar Series & Summary
Hosted by PHI’s Center for Connected Health Policy in the fall of 2021, this webinar series explores the rapid, ever-changing and complex landscape for telehealth policy in Medicaid, specifically in the context of COVID-19.
The COVID-19 pandemic has caused an increase in telehealth usage, resulting in many temporary telehealth policy changes on the federal and state level. PHI’s Center for Connected Health Policy’s Medicaid & Telehealth: A Policy Webinar Series focused on topics such as audio-only, policies that have been made permanent, and the Medicaid program’s reasoning for those decisions.
Listen to the recordings to learn from high-level experts and administrators representing 7 different Medicaid agencies or other state offices (Arizona, Colorado, Kentucky, North Carolina, Oregon, Tennessee and Vermont).

Speakers discussed the unique approaches they took to crafting and deciding on what telehealth policies to implement and how COVID-19 has impacted recent decisions. Among some of the highlights from this four-week series:
- The thought and efforts state programs had put in to developing policies to meet the needs of their enrollees.
- The different approaches to gathering data to help inform policy changes.
- The steps states have taken toward ensuring people with disabilities are able to access services via telehealth.
Throughout the series, speakers emphasized that telehealth does indeed benefit patients. While states may have taken different approaches and crafted different policies, they all acknowledged the benefit of ensuring telehealth was available in some capacity for their communities to access.
Access the recordings of the webinar series
Telehealth & Medicaid: Medicaid & Audio Only
September 17, 2021
Policymakers on the federal and state level continue to decide which of the temporary telehealth policies to keep after the public health emergency is over. This webinar focuses on the permanent telehealth policy changes Medicaid programs have made and what went into those decisions. See additional resources from the webinar.
Telehealth & Medicaid – Medicaid Telehealth Policy & Data, Evaluations, & Stakeholders
September 24
COVID-19 has spurred Medicaid programs to expand their telehealth policies. It has also encouraged them to examine the effects and impacts of such policies and engaging stakeholders more often than before. Learn about the efforts some Medicaid programs have made in collecting data and working with other groups as they work on solidifying the next steps in their telehealth policy development. See additional resources from the webinar.
Telehealth & Medicaid – Telehealth & Patients with Disabilities
October 1
As telehealth became more widely utilized during COVID-19, it became clear that some segments of the population may be left behind due to inability to access the technology. One segment of the population, patients with disabilities, may have encountered unique barriers to accessing care through telehealth. This webinar focuses on what Medicaid programs and other state agencies have done to help ensure people with disabilities can utilize telehealth. See additional resources.
Telehealth & Medicaid – Medicaid Telehealth Permanent Policies
October 8
Policymakers on the federal and state level continue to decide which of the temporary telehealth policies to keep after the public health emergency is over. This webinar explores the permanent telehealth policy changes Medicaid programs have made and what went into those decisions. See additional resources.
The Center for Connected Health Policy (CCHP) has also issued a summary report of the Fall series. To watch recordings of webinars held within the Winter and Spring Medicaid and Telehealth webinar series, visit CCHP’s webinars page or read the respective summary reports of the earlier series, Winter and Spring on CCHP’s reports page.
Video Series: Strong Voices: Black Leaders Who Are Making Neighborhoods Healthier
Meet Black leaders working in community development at the intersection of race, health and poverty, in a video series from PHI’s Build Healthy Places Network and Purpose Built Communities.
Meet Black leaders who are working in community development at the intersection of race, health and poverty, in a video series from PHI’s Build Healthy Places Network and Purpose Built Communities.
The series aims to elevate Black leaders in community development through storytelling, showcasing their leadership style and contributions to the field as members of the Purpose Built Communities Network.
Watch the full series here
Craig Glover, Executive Director of Northend RISE in West Palm Beach, FL
The third and final video in the series features Craig Glover, Executive Director of Northend RISE in West Palm Beach, FL describing how partnerships to elevate the health of the Northend RISE community are shaping health outcomes and enhancing quality — and even quantity — of life for residents.
Regina Hall, Executive Director of Boston-Thurmond United
The second interview in the series features Regina Hall, Executive Director of Boston-Thurmond United in Winston Salem, NC, conducted by Zachary Travis, Research Associate of Build Healthy Places Network. Regina shares strategies and approaches that have helped engage partners who provide access to critical healthcare resources for residents of the Boston-Thurmond neighborhood.
Danny Shoy, President and CEO of the East Lake Foundation
The first interview in the series features Danny Shoy, President and CEO of the East Lake Foundation, conducted by Zachary Travis, Research Associate of Build Healthy Places Network. Shoy shares how community wellness shaped his resident-centered approach, which helps make the East Lake neighborhood a place where residents live longer, healthier lives.
Learn more about the series:
Video Series: Promising Practices for Equitable Vaccine Distribution
This video series, from PHI’s Public Health Alliance of Southern California, showcases community-informed and equity-centered practices that reach disproportionately impacted low-income communities and communities of color.
Created by PHI’s Public Health Alliance of Southern California, this video series elevates promising and replicable practices for equitable vaccine distribution. The videos showcase real-life community-informed and equity-centered practices that reach disproportionately impacted low-income communities, and communities of color.
Reaching Native Hawaiian & Pacific Islanders in Vaccine Distribution (6/17/2021)
Recognizing the longstanding challenges that NHPI communities have faced, the Utah Pacific Islander Health Coalition (UPIHC), in partnership with several local health departments, like the Utah County Health Department, and the Utah State Health Department, mobilized early to begin hosting weekly vaccination clinics focused on increasing access to vaccinations for NHPI community members in a safe, trusting, and culturally affirming way. Many of the mobile vaccination clinic efforts aimed at reaching NHPI community members in Utah are coordinated partnerships through the UPIHC member network. The mobile vaccination clinics are tailored to create a space that is culturally grounded, and feels safe and comfortable for the NHPI community, which includes partnering with faith-based partners and hosting clinics in familiar locations. The partnership efforts between Utah’s local health departments (LHDs) and UPIHC has been a leading factor behind the distribution of 1,000’s of vaccines to the NHPI community throughout the State.

Reaching Transgender Community Members in Vaccine Distribution (5/13/2021)

Improving Vaccination Accessibility for Individuals Living with Disabilities (4/16/2021)
 Health leaders from The Los Angeles County Department of Public Health’s (LADPH) Center for Health Equity, in partnership with key community stakeholders with lived experience and organizations that serve communities with disabilities, have developed and are working to implement a set of core recommendations to improve access to COVID-19 vaccinations for individuals living with disabilities. The recommendations developed are a recognition of the urgent need to develop processes and systems to improve accessibility for communities with disabilities throughout Los Angeles County. While the recommendations address current COVID-19 vaccination efforts, these recommendations may be applied to COVID-19 testing and broader emergency response activities. In this video, we are joined by Heather Jue Northover, LADPH Center for Health Equity Director and Hector Ochoa, Director of Public Policy for the Southern California Resource Services for Independent Living, as they discuss the importance of centering individuals with lived experience in designing vaccine distribution solutions that truly work for all.
Health leaders from The Los Angeles County Department of Public Health’s (LADPH) Center for Health Equity, in partnership with key community stakeholders with lived experience and organizations that serve communities with disabilities, have developed and are working to implement a set of core recommendations to improve access to COVID-19 vaccinations for individuals living with disabilities. The recommendations developed are a recognition of the urgent need to develop processes and systems to improve accessibility for communities with disabilities throughout Los Angeles County. While the recommendations address current COVID-19 vaccination efforts, these recommendations may be applied to COVID-19 testing and broader emergency response activities. In this video, we are joined by Heather Jue Northover, LADPH Center for Health Equity Director and Hector Ochoa, Director of Public Policy for the Southern California Resource Services for Independent Living, as they discuss the importance of centering individuals with lived experience in designing vaccine distribution solutions that truly work for all.
Read: Improving Vaccination Accessibility for Individuals Living with Disabilities
Health and Housing in St. Louis (3/29/2021)
 The City of St. Louis Health Department partnered with the St. Louis Housing Authority to help register hard hit communities for COVID-19 vaccination. In St. Louis, data from a January 2021 survey revealed that of 17,000 individuals who registered their interest in receiving the COVID-19 vaccine, less than 3,000 were from under-resourced and low-income neighborhoods such as North St. Louis.
The City of St. Louis Health Department partnered with the St. Louis Housing Authority to help register hard hit communities for COVID-19 vaccination. In St. Louis, data from a January 2021 survey revealed that of 17,000 individuals who registered their interest in receiving the COVID-19 vaccine, less than 3,000 were from under-resourced and low-income neighborhoods such as North St. Louis.
Leaders like Dr. Fredrick Echols with the City of St. Louis Department of Health were proactive in outreach to communities most disproportionately impacted by the COVID-19 pandemic. Partnering with Alana Green, Executive Director of the St. Louis Housing Authority, and staff from their Resident Initiatives Team, they called residents and assisted them in setting up vaccine appointments. Engaging the Housing Authority as a trusted partner and messenger for this community resulted in vaccinating over 300 seniors in just one clinic effort, roughly 98% of whom identified as Black/African American! An invite only follow-up vaccination clinic with Housing Authority residents resulted in a 96.3% return rate for the second dose of COVID vaccinations. The partnership between the Health Department and Housing Authority has yielded other promising benefits to housing authority residents, including food distribution, and distribution of personal protective equipment. This partnership serves as a promising model for intra-governmental partnerships to reach disproportionately impacted community members in vaccine distribution and administration.
Read: Intra-Governmental Partnerships to Reach City of St. Louis Housing Authority Residents
Protect Chicago Plus (3/18/2021)

In January 2021 Chicago City Mayor Lori Lightfoot announced Protect Chicago Plus, a targeted COVID-19 vaccination distribution program designed with equity as the central strategy to ensure that vaccines are reaching communities hardest hit by the COVID-19 pandemic.
Protect Chicago Plus is a unified effort between the City of Chicago, the Chicago Department of Public Health (CDPH), and local community partners with the goal of changing the map of disease burden and ending the pandemic. The City’s efforts have successfully increased the percent of 1st dose vaccines going to Black and Latinx Chicagoans from 18% in the first week of distribution to close to 59% in the most recent week of distribution (as of March 9, 2021); a percent equal to the City’s total Black and Latinx population. In light of their early successes, partners in Chicago remain steadfast in their commitment to lead with equity in vaccine distribution.
Read: Data-Driven, Neighborhood-Based Strategies to Reach Black and Latinx Chicagoans
Riverside Vaccinates Farmworkers (3/9/2021)
 Riverside County Public Health Department, in partnership with the Coachella Valley Equity Collaborative (spearheaded by the Desert Healthcare District & Foundation (DHCD) and community-based partners, like TODEC), launched mobile vaccination clinics that brought COVID-19 vaccines directly to farmworkers in the fields.
Riverside County Public Health Department, in partnership with the Coachella Valley Equity Collaborative (spearheaded by the Desert Healthcare District & Foundation (DHCD) and community-based partners, like TODEC), launched mobile vaccination clinics that brought COVID-19 vaccines directly to farmworkers in the fields.
Community-based partners helped register farmworkers, who have been some of the most impacted community members due to COVID-19, at their worksites. They also worked to answer questions in preferred languages, including indigenous languages such as Purepecha. Partners in these efforts worked to address a broad range of concerns during vaccine registration and administration, including concerns related to vaccine side effects, immigration status and public charge. To date, the mobile vaccination clinics have successfully vaccinated well over 5,000 farmworkers throughout the Eastern Coachella Valley (and counting!). These successful efforts have also been elevated by the State as promising practices to replicate across California. This collaboration was made possible with funding support from the Public Health Institute’s Together Toward Health Initiative.
Black and Well in the LBC (3/3/2021)
 Early on in the pandemic, the City of Long Beach Health Department was acutely aware of the disparate impacts that the COVID-19 pandemic was having on low-income communities and communities of color throughout the City, especially Black, Latinx, and Cambodian communities. Moreover, early COVID-19 vaccination data revealed that the hardest-hit communities were not getting vaccinated at the same rates as less impacted communities. In an effort to ensure more equitable distribution of the COVID-19 vaccine, the City has launched a series of partnerships with community-based organizations to host mobile vaccination clinics aimed at reaching Black, Latinx and Cambodian community members.
Early on in the pandemic, the City of Long Beach Health Department was acutely aware of the disparate impacts that the COVID-19 pandemic was having on low-income communities and communities of color throughout the City, especially Black, Latinx, and Cambodian communities. Moreover, early COVID-19 vaccination data revealed that the hardest-hit communities were not getting vaccinated at the same rates as less impacted communities. In an effort to ensure more equitable distribution of the COVID-19 vaccine, the City has launched a series of partnerships with community-based organizations to host mobile vaccination clinics aimed at reaching Black, Latinx and Cambodian community members.
“Black and Well in the LBC” was a one-day mobile vaccination clinic held on Wednesday, February 10th, hosted in partnership with the City, the Long Beach Health Department, community-based non-profit Elite Skills Development and The Long Beach Minister’s Alliance. The vaccination event was held in Central Long Beach, a historically Black community, with a goal of reaching older Black Long Beach residents. The creation of this culturally affirming space, with trusted community partners in the lead, resulted in setting up vaccination appointments for 200 people, of which approximately 95% identified as Black or African American.
Telehealth & Medicaid: A Spring 2021 Policy Webinar Series & Summary
Hosted by PHI’s Center for Connected Health Policy in the spring of 2021, this webinar series focused on the rapid telehealth policy ever-changing and complex landscape for telehealth policy in Medicaid, specifically in the context of COVID-19. See the recordings and report summary.
COVID-19 has forever changed many aspects of our lives, including how health care is delivered. With the arrival of the pandemic, a quick pivot to the use of telehealth to provide services was made, necessitating in many temporary telehealth policy changes on the federal and state level. Much attention has been paid to federal Medicare telehealth policy changes, but there has been less focus on the actions taken by state Medicaid programs.
PHI’s Center for Connected Health Policy’s (CCHP) Medicaid telehealth policy webinar series addresses this gap in knowledge and also provides a forum for states to share their innovative work on telehealth policy and engage with other state Medicaid programs.
With nine Medicaid programs participating, the purpose of the Spring 2021 Series was to examine specific areas of telehealth policy and their impacts on particular patient populations. Participating in the series were representatives from Medicaid programs in California, Connecticut, Georgia, Kansas, Massachusetts, Minnesota, New York, Texas, and Washington.
Listen to the recordings to learn from high-level experts and administrators representing 10 different Medicaid agencies, as well as experts from the federal Centers for Medicare & Medicaid Services and Medicaid and CHIP Payment and Access Commission.

Speakers discussed the policies they have instituted during the pandemic that impacted the aforementioned areas and what temporary policies they will, or are considering, retaining. For some of the programs, their general telehealth policies applied to all populations, but a few did note that some services may have been more difficult to deliver via technology depending on age. For example, very young children may have been more difficult to examine via technology than an older child who may have been more willing to sit still during a telehealth encounter. As with other Medicaid programs, many of the speakers noted the significant use of telehealth to deliver mental and behavioral health services.
Access the recordings of the webinar series
- Access and Equity in Medicaid Telehealth Policy
- Medicaid Telehealth Policies for Children and Youth
- Medicaid Telehealth Policies for Seniors
- Telemental Health & State Medicaid Policies
Report: Telehealth & Medicaid: A Policy Webinar Series
CCHP also completed and released a report summarizing the four webinars hosted during the Spring series. The report dives into the findings gleaned from the presentations and synthesizes key takeaways from each Medicaid agency’s COVID-19 telehealth policy activities.

Register for the Fall 2021 Policy Webinar Series: Telehealth & Medicaid
PHI’s Center for Connected Health Policy is hosting their second Telehealth & Medicaid: A Policy Webinar Series, returning in April with four new webinars exploring telehealth and Medicaid in the context of COVID-19, and featuring Medicaid experts. These four webinars will be held in September/October and will explore the topics of Medicaid & Audio-Only; Medicaid & Telehealth Data Collection: Surveys, Studies & Advisory Groups; Medicaid & Other State Agencies Telehealth Policies for Patients with Disabilities; and Medicaid & Permanent COVID-19 Telehealth Policies.
Web Forum Series: Hesitancy, Equity & Transparency in the COVID-19 Vaccine Roll Out
This Web Forum series, from PHI’s Dialogue4Health, explores how policymakers, health care providers, pharmacies, and community-based organizations can build trust, address population-specific needs, leverage trusted community resources and more.
Trust and trustworthiness are a significant part of achieving equitable distribution of COVID-19 vaccines. Watch the recordings from this Dialogue4Health Web Forum series to explore issues related to building trust and trustworthiness between communities and those bringing vaccines.

In a previously recorded, live conversation, PHI CEO & President Dr. Mary Pittman and Pastor James D. Gailliard, a state representative in the North Carolina Assembly, reflect upon efforts to achieve equitable distribution of COVID-19 vaccines and explore how faith-based organizations and state policy interventions work toward this goal in North Carolina.
In this web forum, speakers address:
- Issues related to building trust and trustworthiness between communities and those bringing vaccinations to the communities;
- Successful strategies for reaching vaccine-hesitant communities;
- How data can be used to ensure an equitable vaccine response;
- How vaccine distribution strategies have evolved as supply increases; and
- What we have learned about how to build stronger and lasting relationships between communities and public health in preparation for the next pandemic or natural disaster.
Hesitancy, Equity, and Transparency: Rolling out the COVID-19 Vaccine (5/6/2021)
In this previously-recorded Dialogue4Health Web Forum, moderator Dr. Mary Pittman, PHI CEO & President, and speakers—including Dr. Bechara Choucair, Vaccinations Coordinator for the White House COVID Response Team, responsible for overseeing the national vaccination efforts under the Biden-Harris administration—discuss strateiges for how policymakers, health care providers, pharmacies, and community-based organizations can build trust, address population-specific needs, leverage trusted community resources and more.
In this web forum, speakers address:
- Issues related to building trust and trustworthiness between communities and those bringing vaccinations to the communities;
- Successful strategies for reaching vaccine-hesitant communities;
- How data can be used to ensure an equitable vaccine response;
- How vaccine distribution strategies have evolved as supply increases; and
- What we have learned about how to build stronger and lasting relationships between communities and public health in preparation for the next pandemic or natural disaster.
Webinar Recording: DDT Exposure in Grandmothers Linked to Obesity, Earlier Periods in Granddaughters
New Meaning of “Persistence” for an Environmental Chemical Banned 50 Years Ago
In this webinar, Dr. Cohn, director of PHI’s Child Health and Development Studies, discussed her recent research which found that young women today may face increased health risks linked to breast cancer due to their grandmothers’ exposure to the banned pesticide DDT.
Learn more about the studyThis was the first study to report on the health effects of exposure to a toxic environmental chemical over three human generations, and found that granddaughters whose grandmothers were exposed to the pesticide DDT have higher rates of obesity and earlier first menstrual periods. This may increase the granddaughters’ risk for breast cancer as well as high blood pressure, diabetes and other cardiometabolic diseases.
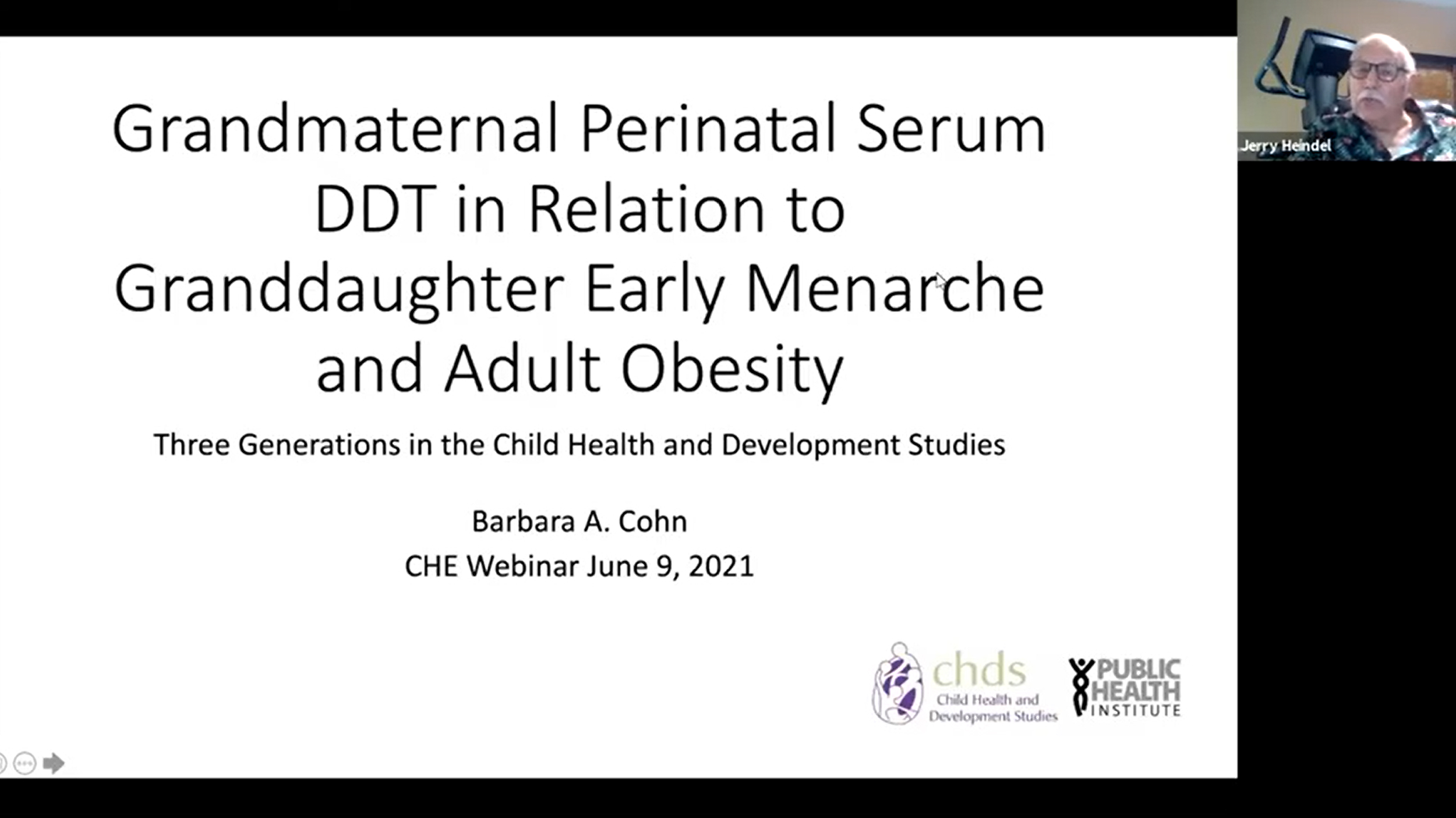
This research was conducted by PHI’s Child Health and Development Studies where 15,000 pregnant women donated blood samples during and shortly after their pregnancies in the 1960s. These women have been followed for their own health and the health of their daughters and granddaughters for over 60 years.
This work is the first to show such a 3 generation effect for a pesticide in humans and gives new meaning to the idea of “forever” chemicals. Dr. Cohn discussed what this study means for current generations of women and current environmental issues.
This webinar is one in a monthly series sponsored by the Collaborative on Health and the Environment’s EDC Strategies Partnership.

Featured Speaker: Barbara A. Cohn
Barbara A. Cohn, PhD, is director of the Child Health and Development Studies (CHDS) at PHI. CHDS is home to a groundbreaking study, which originated in 1959, designed to shed light on the various factors impacting health during pregnancy and early childhood. Between 1959 and 1967, 15,000 pregnant women and their families were enrolled. Researchers continue to study these rich data and conduct important follow-up studies to further examine how events during pregnancy impact the subsequent health of fathers, mothers and their children and grandchildren. Cohn consults with researchers around the world on the use of the CHDS data for health research.
In addition, Cohn directs research examining how pregnancy protects against breast cancer and influences other health problems in mothers and their children in order to identify natural protective mechanisms that can be used for prevention. She also investigates whether early life exposure to environmental chemicals during pregnancy affects obesity, immune function, reproductive health, cardiovascular disease, diabetes, neurodevelopment, cancer, and health disparities in mothers and their children across the life span.
Cohn holds a doctorate in epidemiology, a master’s degree in city and regional planning, a master’s degree in public health planning and a bachelor’s degree in zoology, all from the University of California, Berkeley.
Webinar: Partnering with Communities to Navigate Equitable Vaccine Access
In this CDC Foundation webinar, presenters discuss their work with community-based organizations, as they collaborate on ways to navigate what can be a difficult path toward getting the community vaccinated. Featuring Susan Watson, director of PHI’s Together Toward Health.
The rollout of the COVID-19 vaccines offers a big dose of hope toward ending the pandemic that has wreaked havoc on the nation. But for many underserved communities—some of the hardest hit by the pandemic—accessing those vaccines remains a challenge all its own.
In this CDC Foundation webinar, featuring Susan Watson, MPH, Director of PHI’s Together Toward Health, presenters discuss their work with community-based organizations (CBOs), as they collaborate on ways to navigate what can be a difficult path toward getting the community vaccinated. Presenters also share strategies to address the concerns and needs of communities, and to overcome the challenges of getting people vaccinated. This webinar is part of a CDC Foundation special series specifically tailored to CBOs and their partners.
Telehealth & Medicaid: A Winter 2021 Policy Webinar Series & Summary
Developed by PHI’s Center for Connected Health Policy, this webinar series focuses on the rapid telehealth policy ever-changing and complex landscape for telehealth policy in Medicaid, specifically in the context of COVID-19.
Created by PHI’s Center for Connected Health Policy (CCHP), Telehealth & Medicaid: A Policy Webinar Series was developed in response to an ever-changing and complex landscape for telehealth policy in Medicaid, specifically in the context of COVID-19.
Listen to the recordings to learn from high-level experts and administrators representing 10 different Medicaid agencies, as well as experts from the federal Centers for Medicare & Medicaid Services and Medicaid and CHIP Payment and Access Commission.
Because Medicaid programs are administered at the state level, no two Medicaid programs are alike. Under federal law, Medicaid programs are required to provide a set of essential services, which includes a variety of preventive, inpatient, and outpatient healthcare services but excludes services like dental, optometry, or specialty care, among others. States elect to cover optional benefits above and beyond the MEC guidelines. Similarly, Medicaid programs have discretion in determining the scope of their telehealth coverage policies. While states have increasingly moved to reimburse providers for telehealth services in recent years, telehealth coverage policies can range from narrow to expansive.
As Medicaid programs rapidly expanded their telehealth coverage policies amidst the COVID-19 pandemic, PHI’s Center for Connected Health Policy CCHP developed a policy tracking tool that captures the COVID-related telehealth policy actions for Medicaid programs in all 50 states and the District of Columbia (DC). The Medicaid webinar series is an extension of this work and offered providers, administrators, and policy staff in Medicaid agencies the opportunity to share insights and best practices with a diverse audience.
Access the recordings of the webinar series
- Waivers and State Plan Amendments to Address COVID-19
- Provider Engagement & Education During the Public Health Emergency
- Patient Engagement & Education During the Public Health Emergency
- What’s Next? A Roadmap for Medicaid Telehealth Policy Beyond the Pandemic
Report: Telehealth & Medicaid: A Policy Webinar Series
CCHP also recently completed and released a report summarizing the four webinars hosted during the Winter series. The report dives into the findings gleaned from the presentations and synthesizes key takeaways from each Medicaid agency’s COVID-19 telehealth policy activities.
Register for the Fall 2021 Policy Webinar Series: Telehealth & Medicaid
PHI’s Center for Connected Health Policy is hosting their second Telehealth & Medicaid: A Policy Webinar Series, returning in April with four new webinars exploring telehealth and Medicaid in the context of COVID-19, and featuring Medicaid experts. These four webinars will be held in September/October and will explore the topics of Medicaid & Audio-Only; Medicaid & Telehealth Data Collection: Surveys, Studies & Advisory Groups; Medicaid & Other State Agencies Telehealth Policies for Patients with Disabilities; and Medicaid & Permanent COVID-19 Telehealth Policies.
“Is COVID-19 Outpacing Test and Contact Tracing?” Podcast with Marta Induni of PHI’s Tracing Health Program
On this podcast episode of “A Shot in the Arm,” Dr. Marta Induni of PHI’s Tracing Health program discusses whether COVID-19 testing and contact tracing programs are reaching the people in need, what have we learned, and where we go from here.
In the latest “Shot in the Arm” podcast, PHI’s Dr. Marta Induni gives an update on the Tracing Health program and discusses contact tracing in the communities most impacted by COVID-19. The series on COVID-19 is a collaboration between the podcast and the Bay Area Global Health Alliance.
“We teach our staff through ‘trauma informed training.’ We are working with traumatized communities and our contact tracers are from those communities.”
Dr. Marta Induni, Tracing Health

A Shot in the Arm podcast
You can also watch Mary Pittman, PHI President and CEO and Board Chair of the Bay Area Global Health Alliance discussing “COVID-19: Public Health on the Line” on a previous episode of the Shot in the Arm podcast.
Connecting Public Health, Policy, & Equity in COVID-19: An Executive Conversation
In 2020, amidst COVID-19 racial health disparities and modern movements of social justice, leaders and policymakers were challenged to discuss equity and commit to meaningful action. Watch PHI President Mary Pittman, IMPAQ President and PHI Board Member Adaeze Enekwechi, and Academy Health President Lisa Simpson to hear how leaders are grappling with issues of health equity during the COVID-19 crisis and where they see opportunities for progress.
The racial health disparities of the COVID-19 pandemic, combined with one of the most significant modern movements for social justice, have made 2020 a year for leaders and policymakers to ask tough questions about equity and commit to meaningful action.
In a previously recorded, live conversation with PHI’s President and CEO Mary Pittman, DrPH, IMPAQ President and PHI Board Member Adaeze Enekwechi, PhD, MPP, and Academy Health President Lisa Simpson, MB, MCh, MPH, FAAP hear first-hand how leaders from across the spectrum of research, policy, and practice are grappling with issues of health equity during the COVID-19 crisis and where they see opportunities for progress.
Work With Us
You change the world. We do the rest. Explore fiscal sponsorship at PHI.
Support Us
Together, we can accelerate our response to public health’s most critical issues.
Find Employment
Begin your career at the Public Health Institute.
