
Across the country, no two states are alike in how they define and regulate telehealth. To help policymakers, health advocates and other health care professionals understand the policies and trends throughout the nation, the Telehealth Policy Finder tool compiles telehealth-related laws and regulations across all 50 states and the District of Columbia, as well as at the federal level.
Explore the Policy Finder toolAs some states have implemented targeted exceptions from licensing requirements for out-of-state telehealth providers since Fall 2023 (as discussed above), other states have implemented special registrations or licensure processes for out-of-state telehealth providers, allowing an alternative process to full in-state licensure to offer telehealth services within the state in certain instances and subject to specific requirements. Twenty-two states, as well as the Virgin Islands now offer special telehealth licenses, or registration processes for out-of-state providers. To be counted in this number, the licenses/registrations did need to specifically reference telehealth (or remote care) in some way. A recent state to implement this is Arizona, which introduced new regulations (implementing a previously passed law) that establishes a telehealth provider registration process for out-of-state providers, outlining practice standards such as consent and liability insurance requirements within it. In Washington, SB 5481 enacted the Uniform Telehealth Act, which in addition to adopting limited licensure exceptions for out-of-state providers, encourages a review of the Uniform Law Commission’s proposal for an out-of-state provider registration process, signaling the state’s interest in developing a more formalized approach. Delaware also adopted regulations that allow social workers practicing via interstate telehealth to bypass the need for a full Delaware license if they are registered under the state’s telehealth registration system.
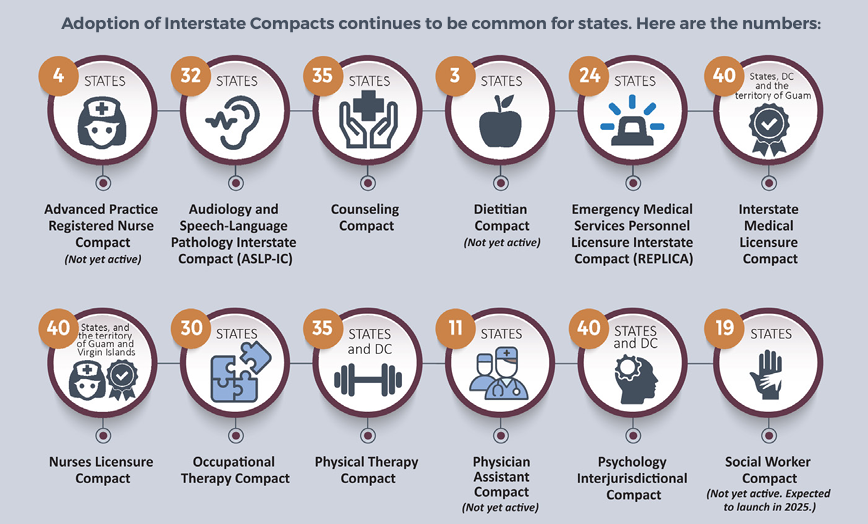
Although states have introduced specific provisions for out-of-state providers, interstate compacts remain the most common method for enabling out-of-state practitioners to work across multiple professions and states. These compacts typically allow specific healthcare providers to practice in states where they are not licensed, provided they hold a valid license in their home state, and possess a special ‘compact’ license. Currently, CCHP monitors twelve different Compacts, each with its own distinct eligibility criteria and process. For instance, the Interstate Medical Licensure Compact streamlines the licensure process, although physicians are still required to apply for licenses in individual states. We saw the largest jump in participation in the Social Work Compact, Counseling Compact and Physician Assistant Compact during this Fall 2024 edition of the report. Since last year, a new Compact was also added to CCHP’s tracking, the Dietitian Compact. So far, only three states (Alabama, Nebraska and Tennessee) are member states. In addition, as some compacts are relatively new, not all are currently considered active and/or issuing licenses at this time.
Read the full Fall 2024 report, and explore the state summary chart showing where states stand on many key telehealth policies, as well as an infographic highlighting key findings.

CCHP has added an Out-of-State Telehealth Providers policy trend map to the CCHP website which color codes states based on the presence of limited licensure exceptions, telehealth registration processes, or both. This webpage also provides a link to CCHP’s Interstate Licensure Compacts information, showing Compact participation status by state.
Launched in Spring 2021 by PHI’s Center for Connected Health Policy (CCHP), the Policy Finder tool is a searchable, easy-to-use database that is updated consistently throughout the year. Formerly known as the State Telehealth Laws and Reimbursement Report, the information from the online database can be exported for each state into a PDF document using the most current information available on CCHP’s website.
The Policy Finder is designed to provide timely policy information that is easy for users to navigate and understand. Watch a quick tutorial to explore the tool, see how to use it and learn about its features:
Please note: this information should not be construed as legal counsel. Consult with an attorney if you are seeking a legal opinion.
Originally published by Center for Connected Health Policy
You change the world. We do the rest. Explore fiscal sponsorship at PHI.
Together, we can accelerate our response to public health’s most critical issues.
Begin your career at the Public Health Institute.

Communities across the U.S. and around the world are grappling with dangerous wildfires and extreme heat. Explore PHI's resources, tools, programs and impacts to help protect your community—with a focus on ways to reach systemically excluded groups with key resources and information, and invest in transformative solutions to promote safety, equity and resiliency.

